You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Clear Skin Diet by Nina Nelson PDFDocument370 pagesThe Clear Skin Diet by Nina Nelson PDFmia agustina60% (10)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Odors of Santity Distinctions of The Holy in Early Christianity and IslamDocument13 pagesOdors of Santity Distinctions of The Holy in Early Christianity and Islamkiedd_04100% (1)
- Cell PhysiologyDocument61 pagesCell Physiologykiedd_04100% (4)
- Nueva Ecija Mental Health StatusDocument27 pagesNueva Ecija Mental Health StatusJRABNENo ratings yet
- "Traditional" Exegeses of Q 4:34Document15 pages"Traditional" Exegeses of Q 4:34kiedd_04No ratings yet
- The Place For Others in IslamDocument27 pagesThe Place For Others in Islamkiedd_04No ratings yet
- Iklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012Document2 pagesIklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012kiedd_04No ratings yet
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocument25 pagesFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04No ratings yet
- Refleks ArcsDocument34 pagesRefleks Arcskiedd_04100% (1)
- SYNAPSEDocument35 pagesSYNAPSEkiedd_04100% (3)
- Microbiology Colour Plate No.3Document1 pageMicrobiology Colour Plate No.3kiedd_04No ratings yet
- Fadhilat Surah at TakwirDocument1 pageFadhilat Surah at Takwirkiedd_04No ratings yet
- Microbiology Colour Plate No.9Document1 pageMicrobiology Colour Plate No.9kiedd_04No ratings yet
- Microbiology Colour Plate No.8Document1 pageMicrobiology Colour Plate No.8kiedd_04No ratings yet
- Microbiology Colour Plate No.7Document1 pageMicrobiology Colour Plate No.7kiedd_04No ratings yet
- Microbiology Colour Plate No.6Document1 pageMicrobiology Colour Plate No.6kiedd_04No ratings yet
- Microbiology Colour Plate No.5Document1 pageMicrobiology Colour Plate No.5kiedd_04No ratings yet
- Microbiology Colour Plate No.2Document1 pageMicrobiology Colour Plate No.2kiedd_04No ratings yet
- Microbiology Colour Plate No.4Document1 pageMicrobiology Colour Plate No.4kiedd_04No ratings yet
- API® CoryneDocument4 pagesAPI® Corynekiedd_04No ratings yet
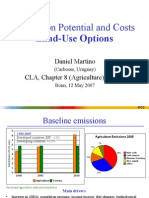
- Mitigation Potential and Costs Land-Use OptionsDocument9 pagesMitigation Potential and Costs Land-Use Optionskiedd_04No ratings yet
- Microbiology Colour Plate No.1Document1 pageMicrobiology Colour Plate No.1kiedd_04No ratings yet
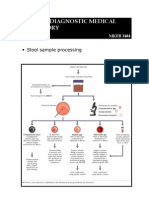
- Stool Sample ProcessingDocument1 pageStool Sample Processingkiedd_04No ratings yet
- Diagram of Classification of EnterobacteriaDocument1 pageDiagram of Classification of Enterobacteriakiedd_04100% (1)
- Mitigation of Climate ChangeDocument25 pagesMitigation of Climate Changekiedd_04No ratings yet
- Philosophical Consolation in Christianity and Islam Boethious and Al-KindiDocument10 pagesPhilosophical Consolation in Christianity and Islam Boethious and Al-Kindikiedd_04No ratings yet
- Mitigation of Climate ChangeDocument41 pagesMitigation of Climate Changekiedd_04No ratings yet
- Advance Diagnostic Medical Laboratory: The AP 20E® For Identification of BacteriaDocument1 pageAdvance Diagnostic Medical Laboratory: The AP 20E® For Identification of Bacteriakiedd_04100% (1)
- Oxidase TestDocument1 pageOxidase Testkiedd_04100% (1)
- Carnitine DeficiencyDocument21 pagesCarnitine Deficiencykiedd_04100% (1)
- Pulmonary Edema Vs Pneumonia OrderDocument25 pagesPulmonary Edema Vs Pneumonia OrderRizqon RohmatussadeliNo ratings yet
- EICT Patient Information Leaflet - Edgbaston - Aug 19Document4 pagesEICT Patient Information Leaflet - Edgbaston - Aug 19el esNo ratings yet
- Family PlanningDocument16 pagesFamily PlanningAnas Abdul SalamNo ratings yet
- DR Adedayo OSHOLOWU - Clinical Director - Special Olympics - NIGERIADocument3 pagesDR Adedayo OSHOLOWU - Clinical Director - Special Olympics - NIGERIAAdedayo OsholowuNo ratings yet
- Germany CV Format-Sample OnlyDocument6 pagesGermany CV Format-Sample Onlydeamhi nursing serviceNo ratings yet
- Dr. Jigar PatelDocument6 pagesDr. Jigar PatelJigar PatelNo ratings yet
- Diabetic RetinopathyDocument36 pagesDiabetic RetinopathyRaúl Plasencia SaliniNo ratings yet
- Goodman and Gilman's The Pharmacological Basis of TherapeuticsDocument105 pagesGoodman and Gilman's The Pharmacological Basis of TherapeuticsDiky PratamaNo ratings yet
- Acute Febrile IllnessesDocument96 pagesAcute Febrile IllnessesHAlid mohammed100% (1)
- Vitiligo Case PaperDocument7 pagesVitiligo Case PaperakashNo ratings yet
- Live-Attenuated Vaccine Scpd9 Elicits Superior Mucosal and Systemic Immunity To Sars-Cov-2 Variants in HamstersDocument24 pagesLive-Attenuated Vaccine Scpd9 Elicits Superior Mucosal and Systemic Immunity To Sars-Cov-2 Variants in HamstersfrehanyaqNo ratings yet
- Case PresDocument22 pagesCase Presandrei jinNo ratings yet
- OBM752 HM Unit-IV NotesDocument34 pagesOBM752 HM Unit-IV NotesRajanNo ratings yet
- NCP Deficit Fluid VolumeDocument4 pagesNCP Deficit Fluid VolumeKingJayson Pacman06No ratings yet
- Wheezing, Bronchiolitis, and BronchitisDocument12 pagesWheezing, Bronchiolitis, and BronchitisMuhd AzamNo ratings yet
- MCQ-Chronic Obstructive Pulmonary DiseaseDocument3 pagesMCQ-Chronic Obstructive Pulmonary DiseaseMittulNo ratings yet
- Nexium Iv (Intravenous Injection and Intravenous Infusion) : Product InformationDocument18 pagesNexium Iv (Intravenous Injection and Intravenous Infusion) : Product InformationErickeeNo ratings yet
- AASMRespiratory Events ScoringDocument19 pagesAASMRespiratory Events ScoringAdam GirardoNo ratings yet
- RecentresumeDocument2 pagesRecentresumeapi-437056180No ratings yet
- NCM 109 Gyne Supplemental Learning Material 1Document25 pagesNCM 109 Gyne Supplemental Learning Material 1Zack Skyler Guerrero AdzuaraNo ratings yet
- 06 Fagiolini 3Document10 pages06 Fagiolini 3gibbiNo ratings yet
- Cardiopulmonary Assessment 2020721956580Document36 pagesCardiopulmonary Assessment 2020721956580Kavya MittalNo ratings yet
- 108 217 1 SMDocument13 pages108 217 1 SMAnastasia FebruestiNo ratings yet
- Hema - PointersDocument5 pagesHema - PointersLUALHATI VILLASNo ratings yet
- Sandra John - Case Scenario On Bulimia NervosaDocument7 pagesSandra John - Case Scenario On Bulimia Nervosasandra0% (1)
- PHARMEVODocument3 pagesPHARMEVOFariha AnsariNo ratings yet
- Introduction To Pathology Infectious DiseasesDocument37 pagesIntroduction To Pathology Infectious DiseasesNirav PatelNo ratings yet
- PresentationDocument15 pagesPresentationUtkarsh KaharNo ratings yet